Cardiac-CT
Computed tomography of the heart
Overview
A cardiac CT scan can visualize the heart muscle, the heart chambers, the heart valves, and, most importantly, the coronary arteries.
Procedure
For a native CT scan without contrast to assess coronary calcification, the patient does not need specific blood test results for the examination. The patient is positioned on the CT table and ECG leads are attached to allow for motion-free image acquisition. After just two breath-hold maneuvers with brief breath-hold phases of less than 10 seconds, the examination is complete, and the patient can leave the CT room after a total of only 5 minutes.
To perform a CT angiography of the heart, an intravenous contrast agent must be administered through a vein in the arm; therefore, a short-term intravenous catheter must be inserted before the examination (similar to a blood draw). Even though the new technology requires only a small amount of contrast agent to be injected for the examination (approx. 60–80 ml, depending on the patient’s weight), any known contrast agent allergy, as well as hyperthyroidism and impaired kidney function, should be ruled out prior to the examination through appropriate blood tests. To improve image quality, patients with an initially higher heart rate may require prior administration of a beta-blocker (metoprolol) to lower the heart rate. A high heart rate causes motion artifacts due to the rapid movement of the coronary arteries, resulting in blurred vessel contours.
Following the native CT scan, the ECG-triggered CT scan is performed during contrast injection using a third breath-hold maneuver (lasting less than 10 seconds) through a narrow section of the chest to visualize the heart alone. For bypass patients, the scan area is expanded to follow the course of the bypass vessels. During the contrast agent injection, you may briefly experience a sensation of warmth in your body as well as changes in taste on your tongue. This is normal and harmless. After the CT scan, the venous cannula is removed and the puncture site is covered with a bandage. The patient may then leave the CT room and go home after receiving a CD with the examination data. The entire examination, including patient preparation, takes only 15–20 minutes.
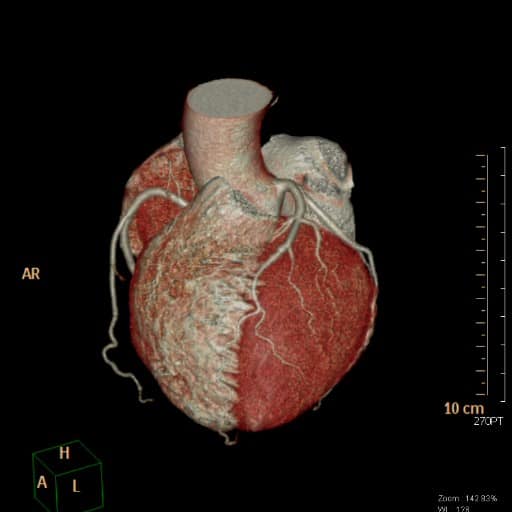


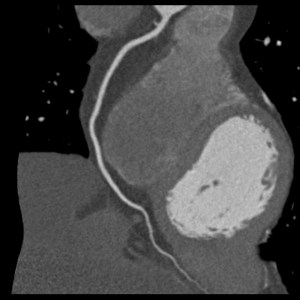
RCA
RCA-Stenose
Calcium Score
A native CT scan performed as part of calcium screening can determine the number and extent of calcifications in the coronary arteries without the use of contrast dye. This procedure is appropriate for patients who have no known history of coronary heart disease and who have no acute symptoms, but who are at some risk (moderate pre-test probability) for coronary heart disease (CHD), e.g., due to high blood pressure, diabetes, high blood lipid levels, family history, or smoking.
The extent of calcification is quantified as a calcium score, calcium mass, and calcium volume, and is used to assess the risk of a cardiovascular event (angina pectoris, heart attack) based on gender and age. Based on the results, the referring primary care physician, internist, or cardiologist can assess the need for further drug therapy. This procedure is not appropriate for patients with symptoms or confirmed coronary artery disease who already have stents or bypasses in place, as it is not possible to make a direct assessment of vessel narrowing without the use of contrast agents.
CT angiography of the coronary arteries
To assess narrowing or blockages in the coronary arteries, an intravenous contrast agent must be administered. Unlike in a cardiac catheterization procedure, however, the iodine-containing contrast agent does not need to be injected directly into a coronary artery via a catheter.
For CT angiography (CTA), a thin, short intravenous line inserted into a vein in the arm is sufficient for administering the contrast agent, so that a simple bandage at the puncture site is all that is needed immediately after the procedure. This eliminates several risks and drawbacks (pressure bandage, hospital stay) associated with cardiac catheterization during CTA, and the patient can go home immediately after the procedure.
CT angiography can be particularly useful for patients without known coronary artery disease who experience unexplained chest pain or shortness of breath, and in whom ECG tests, echocardiography, and blood tests have not provided clear evidence of coronary artery narrowing. Based on our modern CT technology, CT angiography can visualize the coronary arteries in high resolution and without motion artifacts, even while the heart is beating, enabling us physicians to detect not only vessel occlusions but also the severity of a vessel narrowing. This provides a basis for determining whether an invasive cardiac catheterization by a cardiologist is necessary for further evaluation or treatment of the findings identified on the CT scan. Thus, cardiac CT scans can help reduce the need for unnecessary invasive cardiac catheterizations in patients.
This application of cardiac CT has already been recognized as beneficial in a joint consensus statement issued by the German Societies of Cardiology and Radiology. In addition, cardiac CT angiography can be used to non-invasively assess the patency of coronary bypass grafts in previously treated patients. Patients with coronary artery disease who have implanted coronary stents can also be examined using cardiac CT, depending on the type and diameter of the stents; however, the diagnostic value is limited in these patients, particularly for stents smaller than 3.5 mm in diameter and for older metal stents.
Overall, the diagnostic value of CT angiography is limited in cases of severely calcified coronary arteries. For this reason, in our practice we always perform a native CT scan to detect calcification prior to the actual CT angiography, in order to identify patients with severe coronary atherosclerosis and spare them an unnecessary contrast agent injection. Conversely, such patients should be referred for further evaluation via cardiac catheterization.
State of the art
Our new CT technology achieves a low, individually tailored radiation dose while delivering high-quality images of the beating heart through the combination of a state-of-the-art Stellar detector, advanced automatic radiation dose modulation (FAST 3D-Camera, CareKv, CareDose) and high temporal and spatial resolution (128 slices, rotation time 0.33 seconds). This makes it possible to visualize the coronary arteries in particular non-invasively with high image quality.
Analysis
Since early 2025, coronary CT angiography has also been covered for patients with public health insurance when coronary heart disease is suspected.
This requires that the referral from the primary care physician or cardiologist specify the pre-test probability of CHD (which must be between 15% and 70%) and indicate the score used to determine this pre-test probability (e.g., Marburg Heart Score, DISCHARGE Score, ESC Score).
Following the examination, our medical colleagues interpret the cardiac CT scan using specialized software to generate selective images of the coronary arteries and the entire coronary tree. Thanks to the many years of expertise of Dr. Andersen-van Loyen and Mr Singha Roehlen, who specialize in cardiac radiology and have already interpreted several thousand cardiac CT scans, our practice can guarantee outstanding expertise and diagnostic quality.